Here’s How Understanding Heartburn Saves Lives
“Oh, my GERD!” is a very common joke pulled on people suffering from the symptoms of gastroesophageal reflux disease (GERD). What some fail to understand is that acid reflux is a widespread, highly troublesome disease, that can lead to dangerous complications.
There’s a common misunderstanding between heartburn and a heart attack. It is important to realize the difference between the two, while both may kill the person, one is slow whereas the other is fast.
Heartburn is one of the common causes of epigastric burning pain. This can sometimes mimic the retrosternal chest pain of a myocardial infarction. In order to differentiate the two and to eliminate the risk of dismissing a heart attack as a simple heartburn, let us understand heartburn in detail.
Pathogenesis - What Is the Reason Behind Heartburn?
Let us first briefly recollect the normal anatomical and physiological aspects of the stomach that is involved in the disease progression - the lower esophageal sphincter.
LES refers to the circular muscle at the lower end of the esophagus that is 5 cm long and has an intra-abdominal length of about 2 cm.
Normally, when we eat food, the LES relaxes, allowing the food to enter the stomach. To prevent the reentry of contents back into the esophagus, the pressure within the LES builds up, and the sphincter closes. The sphincter normally builds pressures from 6 to 26 mmHg to accomplish this task.
This is where the problem occurs in GERD. The LES fails to close completely, leading to the reflux of contents into the esophagus. The contents are more acidic than the environment of the lower esophagus.
We can consider the LES incompetent if:
- The total length of the LES becomes < 2 cm,
- Intra-abdominal length of the LES becomes < 1 cm, or
- The LES pressure exerted becomes < 6 mmHg.
Factors that increase the risk of GERD and those that have to be avoided in patients with GERD can be easily remembered by the mnemonic - CAPS FAT:
- Coffee and chocolates
- Alcohol
- Peppermint
- Smoking
- Fat
All these factors lower the LES pressure giving rise to GERD.
Other instigating factors of GERD include obesity, pregnancy, age, trauma to the LES, and genetic risks.
So What’s the Damage?
↓
The reflux of the acidic gastric contents leads to an inflammatory reaction at the lower end of the esophagus.
The ulcer and the esophagitis caused by the acid can lead to fibrosis and strictures.
↓
The chronic insult by the acid to the lower esophagus causes metaplasia of the lower esophageal epithelium.
↓
The squamous epithelium of the lower esophagus gets converted to the columnar epithelium (sometimes referred to as intestinal metaplasia).
Such a phenomenon is termed Barret’s esophagus.
↓
If left untreated, this metaplasia can become a full-blown adenocarcinoma of the lower end of the esophagus.

Author: Bruce Blaus
Under the Microscope
There are 3 main histopathological features of GERD:
- Basal cell hyperplasia,
- Elongated connective tissue papillae, and
- Neutrophilic and eosinophilic infiltration
These features are highlighted in the image below.

Author: Nephron
The Patient
Now comes the question, how to identify the diagnosis when we see a patient with epigastric or retrosternal pain, and how to differentiate between heartburn and a heart attack.
| Heartburn | Heart Attack |
| Epigastric pain often without radiation. | Retrosternal pain(The key factor is the radiation of the pain to the neck, jaw, shoulders, arms or the epigastric region). |
| Burning type of pain. | Deep-seated tightness or a squeezing or compressing type of pain. |
| Assess diurnal and postural variations - worsened by postprandial recumbency. | Look for other associated features like sweating, palpitations, and breathing difficulties. |
| Relieved by antacids. | Relieved by nitrates. |
Based on the initial assessment, one can order an EKG to rule out an acute coronary syndrome. Any abnormalities in the EKG (ST elevation, tall or inverted T waves, or any rhythm abnormalities) suggest a cardiac origin of the patient’s symptoms warranting immediate intervention.
A normal EKG, while indicative of GERD, does not rule out an underlying condition. In such a situation, it is often advised to calm the patient down and hold the patient for observation while administering antacids. An EKG can be repeated before sending the patient home (just to be sure).
So How Do We Know for Sure?
Well, the problem is caused by the acidic content of the stomach, so a 24-hour esophageal pH monitoring could be done.
However, esophageal pH or combined esophageal impedance testing is reserved for patients who require surgical intervention and where endoscopy fails to detect esophagitis.
Dealing With GERD
A stitch in time saves nine. Quick lifestyle changes at the right time when appropriately adopted can save the patient a lifetime of trouble. Avoiding or reducing the consumption of caffeine, chocolates, and peppermints and an overall reduction in the amount of fat intake may help in early stages. So does avoiding smoking.
The lack of awareness leads to a delayed presentation with severe symptoms, often requiring intervention using proton pump inhibitors (PPIs) or H2 receptor blockers. These drugs reduce gastric acid production.
Prokinetics can also be used as they promote forward motility of chyme, increasing gastric emptying, and reducing reflux.
Wisdom from Grand Wizard Zeo
“If the patient doesn’t respond to pharmacological therapy, then we should consider surgical management. But let us not be hasty here.
If the patient’s symptoms persist even after treatment with twice-daily proton pump inhibitors, one should think of reassessing the patient for one of the following conditions before considering surgical management:
- Zollinger-Ellison syndrome (ZES) - a gastrinoma causing gastric acid hypersecretion
- Pill induced esophagitis
- Medical non-compliance
Surgical Management
Laparoscopic fundoplication is considered the gold standard for the management of GERD. It is an antireflux technique where the fundus of the stomach is wrapped around the lower end of the esophagus.
There are various modifications of this surgery by various eminent surgeons throughout history:
- Nissen’s fundoplication: 360° wrapping of the esophagus.
- Watson’s procedure: 90° (1/4th of a circle) wrapping of the esophagus anteriorly.
- Toupet’s procedure: 270° wrapping of the esophagus posteriorly.
- Belsey’s fundoplication: 270° wrapping of the esophagus anteriorly.
- Dor fundoplication: 180° wrapping of the esophagus.
The image given below illustrates the Nissen fundoplication.
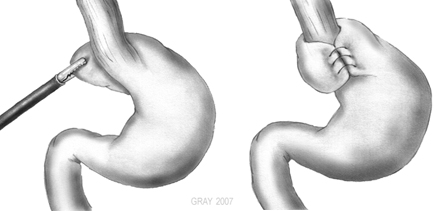
Author: Xopusmagnumx
References:
- Harrison’s Principle of Internal Medicine, 20th edition - Page no: 256 - 259
- Current Medical Diagnosis and Treatment 2020 - Page no: 622 - 626
- https://www.ncbi.nlm.nih.gov/books/NBK430979/
- https://www.ncbi.nlm.nih.gov/books/NBK441938/
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5030713/

Author: DrV
To create awareness about GERD and esophageal cancer
Author’s footnote
While GERD itself has a high prevalence, it can be controlled to a great extent with lifestyle and dietary modifications. Any patient who does not respond satisfactorily to lifestyle modifications and PPIs requires further evaluation to diagnose any underlying pathology such as ZES.
Feel free to click on the references for a more in-depth reading if you so desire.
If you feel any information can be added or that there are any inadvertent errors, feel free to let us know in the comments below or bring it to our notice via support@medicalwizardry.com.
Ever otherwise, feel free to use the comments section for discussion.
We would love to hear from you. Reach out to us via admin@medicalwizardry.com to share any random gibberish/ideas that you would like implemented.