Tuberculosis – Captain Of All These Men Of Death
Introduction
Koch’s disease denotes an infection by Mycobacterium tuberculosis – discovered and announced by Dr. Robert Koch. Also known as tuberculosis (TB), it is a contagious disease that primarily affects the lungs. It would be a grievous mistake to call it a pulmonary pathology, as it can involve almost any part of the body.
In the 1600s, writer John Bunyan penned, “The Captain of all these men of death that came against him to take him away was the Consumption, for it was that that took him down to the grave.”
“Consumption” was a common term to describe tuberculosis in the early days because most patients with tuberculosis waste away and become cachexic.
Several controversies and schools of thought throughout the history of TB and the role of public health, urbanization, poverty, and the standard of living in the spread of TB, as well as its high rate of transmission along with dangerous risks of severe morbidity and mortality, make tuberculosis a vital component of medical history and an important differential diagnosis for a variety of symptoms.

Robert Koch
Pathology
Mycobacterium tuberculosis is usually transmitted by inhalation into the lungs. The air we breathe in is turbulent driving most bacteria into the mucus lining of the airway which is cleaned pretty quickly. M. tuberculosis, however, avoids these mucus traps and makes it into the deeper airways and alveoli of the lungs.
Here, the macrophages phagocytose the tubercular pathogen forming a phagosome. In most cases, the macrophages successfully form a phagolysosome which has hydrolytic enzymes that can breakdown any biomolecule. However, M. tuberculosis produces certain proteins that inhibit the fusion of phagosome and lysosome. Thus, the bacteria survives, proliferates, and creates localized infection. At this point, the patient develops what we call “primary tuberculosis”. Most patients at this stage are asymptomatic but some may have mild flu-like symptoms.
After about 3 weeks of initial infection, cell-mediated immunity kicks in and the immune cells surround the site of tuberculosis infection creating a granuloma. This granuloma walls off the bacteria, preventing its spread. The tissue inside the middle of granuloma undergoes caseous necrosis (cheese-like necrosis as the dead tissue is soft, white, and looks like cheese). This area is known as Ghon focus. Mycobacterium tuberculosis also gets into hilar lymph nodes either carried over by lymph or by direct extension of Ghon focus infection, causing caseation there as well. Together this caseating tissue and associated lymph node make the characteristic Ghon complex. Ghon complex is usually subpleural and occurs in the lower lobe of the lung. The tissue that is encapsulated by granuloma undergoes fibrosis and often causes calcification producing scar tissue that can be seen in an X-ray. This calcified Ghon complex is called the Ranke complex.
Mycobacterium tuberculosis gets killed off by the immune system and that’s the end of that. In some cases even though walled off, they remain viable and dormant (latent). If the patient becomes immuno-compromised in the future due to AIDS, aging, etc., the Ghon focus can become reactivated and the infection can spread to either or both lungs (miliary tuberculosis) as well as can cause a systemic spread through the bloodstream (disseminated TB).
Due to the prior exposure, the immune memory T cells quickly release cytokines, trying to control the new outbreak. This forms cavitating lesions in affected areas of the lung. This can allow the bacteria to disseminate or spread through airways to infect other parts of the lung causing bronchopneumonia. It can also spread by a vascular system and infect every other system in the body causing systemic miliary tuberculosis. As tuberculosis spread to other tissue it causes complications to the organs affected.
TB in other organs
TB can affect any organ, Kidney being commonly affected results in sterile pyuria/increased levels of WBC in the urine. It might spread to meninges causing meningitis, to lumbar vertebrae causing pot disease, adrenal to cause Addison’s disease, liver leading to hepatitis, cervical lymph node to cause lymphadenitis in the neck (scrofula).
Clinical features and Investigation
Patients usually present with symptoms of cough with sputum, fever, night sweats, weight loss, or coughing up blood. Tests for TB must be done in these patients by collecting the coughed out sputum and sending it for lab staining, culture, or PCR. TB can be tested by intradermal skin tests with Purified Protein Derivative, but this can be positive in individuals vaccinated with BCG. Another test for TB is Interferon Gamma Release Assay.
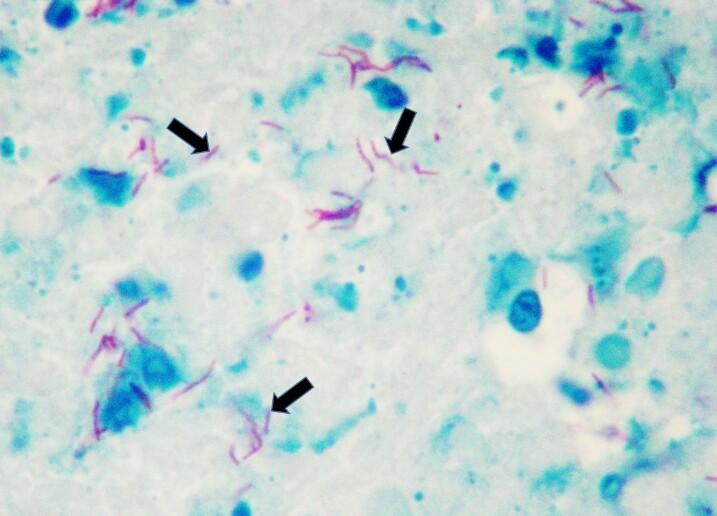
M. tuberculosis (Acid-fast staining)
Management
Treatment of TB involves using combinations of antibiotics which include first-line and second-line antitubercular drugs. First-line drugs include Rifampicin, Isoniazid, Pyrazinamide, and Ethambutol. These drugs given to patients make them noninfectious to others within a few weeks. TB patients are usually kept on medications for 6 months under Directly Observed Treatment Short-course (DOTS) in which a DOTS provider watches and confirms that the patient takes medication. The main goal is to complete the treatment successfully and to control the spread.
References
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5432783/
- https://www.who.int/news-room/fact-sheets/detail/tuberculosis
- https://www.ncbi.nlm.nih.gov/pubmed/7610235
- https://jamanetwork.com/journals/jamainternalmedicine/article-abstract/615670
Author’s footnote
Feel free to click on the references for a more in-depth reading if you so desire.
If you feel any information can be added or that there are any inadvertent errors, feel free to let us know in the comments below or bring it to our notice via support@medicalwizardry.com.
Ever otherwise, feel free to use the comments section for discussion.
We would love to hear from you. Reach out to us via admin@medicalwizardry.com to share any random gibberish/ideas that you would like implemented.