Alzheimer’s Disease – Forgetting The Self
Memory is a way of holding on to the things you love, the things you are, the things you never want to lose - Kevin Arnold
Losing one’s memory is akin to losing a part of themselves. This characteristic feature of Alzheimer’s disease makes it scary.
Alzheimer’s disease (AD) is the most common cause of dementia and the most common neurodegenerative disease.
While this condition is common in the elderly age group and often considered age-related, early-onset has also been observed in middle-aged individuals.
Causes
Age is the primary risk factor for developing Alzheimer's disease. Most of the patients that contract the disease are generally aged above 65 years. Furthermore, the risk of developing Alzheimer's increases exponentially in the 7th and 8th decades of life.
While Alzheimer's is generally not a genetically inherited disease, people who carry the APOE-e4 gene, a sub-type of the APOE gene, are vastly more likely to suffer from Alzheimer's than people who contain the other APOE gene sub-types (e2 and e3).
There are correlations between the levels of education and Alzheimer's disease. The more education a person completes, the less likely he or she is to develop Alzheimer's later in life.
There has also been evidence that women who take estrogen supplements after menopause increase their risk for Alzheimer's.
Furthermore, researchers have found that stroke and heart attack victims are at an increased risk for the disease. Also, high blood pressure, uncontrolled diabetes, and cholesterol levels have been linked to Alzheimer's. Similarly, people who maintain an unhealthy lifestyle put themselves at greater risk.
Pathophysiology
The pathology here in AD is the accumulation of abnormally folded beta-amyloid and tau amyloid proteins in the brain. These proteins disturb the calcium homeostasis and ultimately lead to apoptosis (cell death). This causes the degeneration of the neurons.
AD is also noted to have inflammatory processes and cytokines in the brain, which causes tissue damage. This may add up to the degenerative changes in the brain.
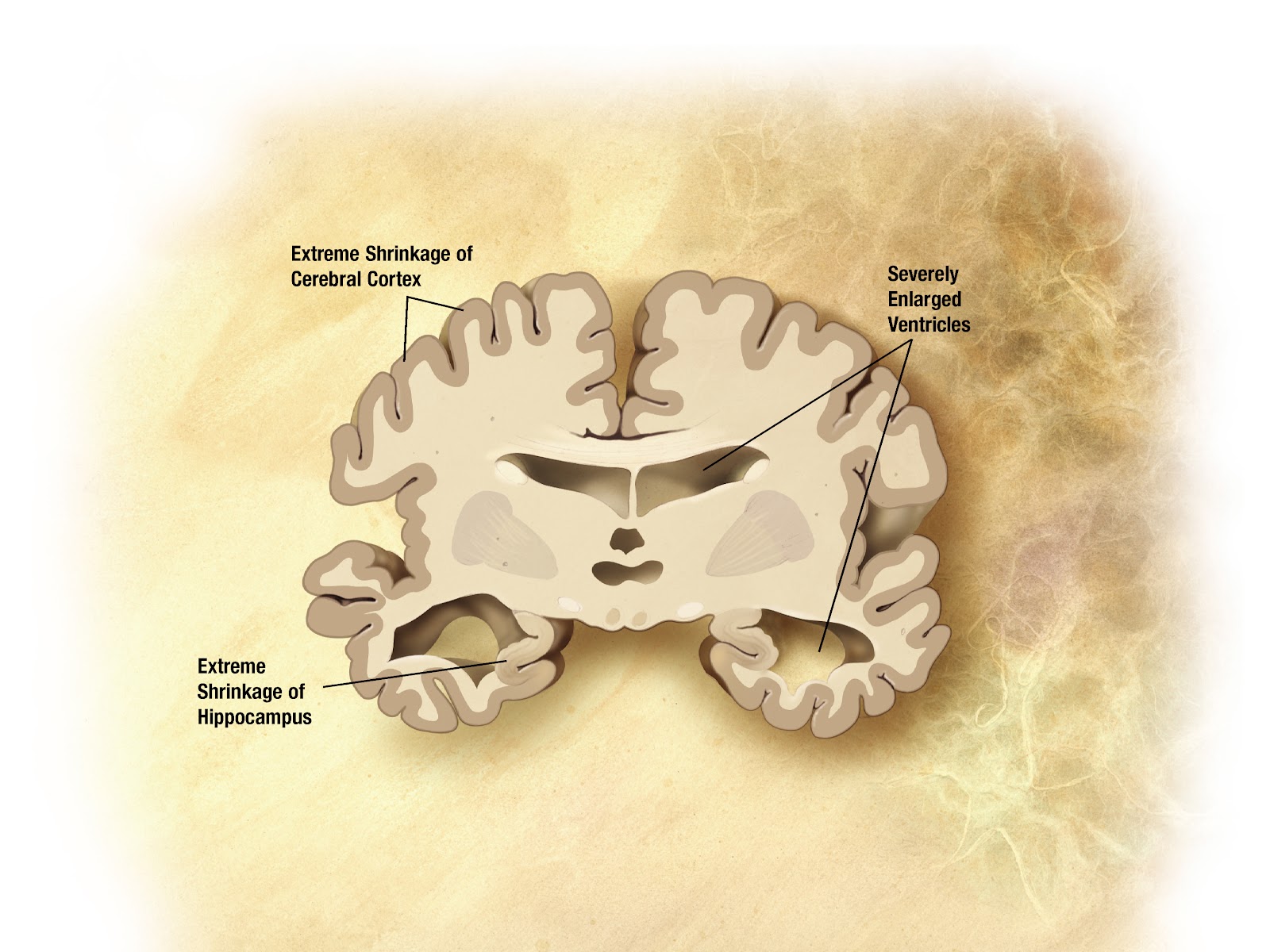
In advanced disease, the brain shows marked shrinkage of the cerebral cortex and hippocampus with enlarged ventricles.
Clinical Features
Patients have a characteristic pattern of cognitive changes, starting with memory loss and advancing to language and visuospatial deficits. Other problems faced by them include,
- Changes in mood
- Misplacing belongings
- Difficulty to complete a familiar task
- Confusion to time and place
- Poor judgment
- Social withdrawal
Neuropsychiatric symptoms can be increased during late afternoon or evening hours (sundowning).
Patients usually present with symptoms according to the stage of the disease.
Stages
AD progresses in 4 stages as follows,
- Mild Cognitive Impairment
- The medial temporal lobe is affected, and patients present with short-term memory loss.
- Mild disease
- The disease involves lateral temporal and parietal lobes. Patients have reading problems, poor direction sense, and recognition of objects becomes difficult for them.
- Moderate disease
- The frontal lobe is affected, and the patient becomes impulsive, not attentive, and has poor judgment.
- Severe disease
- The disease spreads to the occipital lobe with widespread brain atrophy. This produces visual problems, language loss, and motor skill problems in the patient.
Diagnosis
Diagnosis is primarily based on history by the relatives about behavioral observations of the patient.
The triad for diagnosing AD includes
- Slowly progressive decline in memory and orientation.
- Normal biochemical, serological and hematological test results
- Medial temporal lobe atrophy and temporoparietal cortical atrophy as seen in MRI
Criteria
The National Institute of Neurological and Communicative Disorders and Stroke and the Alzheimer’s Association established the most commonly used NINCDS-ADRDA Alzheimer’s criteria for diagnosis.
According to these criteria, to diagnose AD:
- The presence of cognitive impairment and a suspected dementia syndrome has to be confirmed by neurophysiological testing.
- A histopathology confirmation with a microscopic examination of brain tissue is required for a definitive diagnosis of AD.
Other diagnostic methods include advanced medical imaging with CT or MRI. Single-Photon Emission Computed Tomography (SPECT) or Positron Emission Tomography (PET) can be used to exclude other cerebral pathology and subtypes of dementia.
These investigations can also help us in identifying the stage of AD. Assessment of intellectual functioning, including memory testing, can further help us characterize the state of disease.
Management
There is no permanent cure for AD. Treatment aims to give symptomatic relief and to slow down the progression of the disease.
In medical treatment, cholinergic activators like donepezil, rivastigmine, galantamine, and tacrine are used. Memantine, an NMDA receptor antagonist, is also used.
You can remember these drugs with the help of the mnemonic ‘MeGa DoRiTa’
Memantine (the only NMDA receptor antagonist)
Galantamine (cholinergic activator)
Donepezil (cholinergic activator)
Rivastigmine (cholinergic activator)
Tacrine (cholinergic activator)
Other than medical treatment, psychosocial interventions, and palliative treatment is also given for the management of Alzheimer’s disease.
References
- Harrison’s Principles of Internal Medicine, 19th edition, Page no: 2598-2602
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6650620/
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6073093/
Author’s Footnote
Alzheimer’s disease is like a thief that steals all our memories. The person who has the disease will be under a lot of stress. Proper support and caregiving are essential. They must be carefully managed throughout the disease.
Former United States President Ronald Reagan and Irish writer Iris Murdoch were the subjects of scientific articles, examining how their cognitive capacities deteriorated with the course of the disease.
Feel free to click on the references for a more in-depth reading if you so desire. If you feel any information can be added or that there are any inadvertent errors, feel free to let us know in the comments below or bring it to our notice via support@medicalwizardry.com
Ever otherwise, feel free to use the comments section for discussion.
We would love to hear from you. Reach out to us via admin@medicalwizardry.com to share any random gibberish/ideas that you would like implemented.